

If you have a child that is compliant, listens to you, doing well at school, a joy to take out, has no skin or abdominal issues, sleeps well– then this article may not apply to you. When parents decide to change their child’s diet due to behavioural problems or for skin or gastrointestinal issues, for convenience the whole family is often put on the same diet. It is not unusual to have parents return and report that they were surprised to have found other family members that had “no apparent issues” improved as well. I hear of improvements in sleep, bedwetting, improved compliance in other siblings, partners being less “moody” and better to live with. Sometimes the changes may be subtle, but it helps substantially in having a less stressful and more harmonious family environment. Parents are often pleasantly surprised to see the flow on effects of these dietary changes.
Why are there more intolerances to the processed foods we eat? I could present a valid argument along the lines of: when I was growing up (1960’s) most food we ate was made “from scratch”, fruit and vegetables were local, seasonal and very little we ate came from a packet or even a can. Over a relatively short period of years, our children are now eating mainly convenience foods that have been highly processed. Little food is truly made “from scratch”, most snacks are from packets, fruit and vegetables are rarely local and we do not eat seasonally.
What we are feeding our children and ourselves are foods with so many additives and nutritionally depleted that there should be no surprise with the rise in mood disorders and other medical conditions. Even less is talked about the plastic packaging our foods come in. In my day all baby food was packaged in glass. Now baby foods come in plastic squeezable sachets (with attachable plastic spoons), jars, packets, etc. Sad that so many children are growing up not knowing what real food tastes like. Concerning is the amount of chemicals that they are exposed to, ingest and have to process out of their bodies.
Consumption of Artificial Food Colours Over The Years:
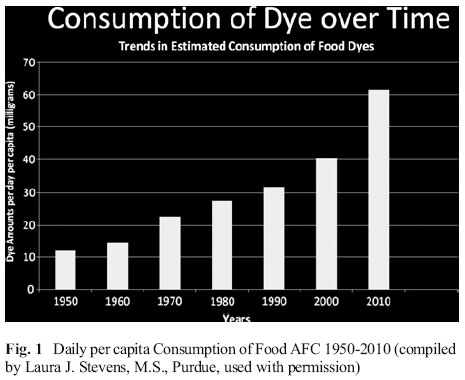
The above table shows the estimated artificial food colour (AFC) consumption per capita in mg/day over the years. It is interesting to see the steep increase between the years 2000 and 2010. So let’s get this into perspective. The amount of artificial food colours being consumed has increased almost 6 times from when I was a child in the 1960’s to 2010! Alarmingly, this consumption in AFCs is increasing rapidly and we have not even considered any other food additives or plasticisers, pesticides, or other environmental pollutants on top of this.
Food Additives and Children’s Behaviour – Is it parental paranoia or is it real?
In the 1960s, American allergist Dr Benjamin Feingold, treating children for skin rashes and other allergic-type reactions, noticed that eliminating certain ingredients from a child’s diet not only improved their skin, but also led to major improvements in their behaviour. He argued the ingredients most likely to be responsible were food additives, such as colourings and preservatives, and naturally occurring chemicals found in plants, called salicylates. Since that time we have had polarised views between those that are passionate about how these chemicals are affecting our health and those that believe that it is just parental or individual’s paranoia.
The effect of artificial food colours on children’s behaviour has now been studied for over 35 years. So you would think we would have a clear answer. Studies are conflicting, and the use of statistics unfortunately confuses the issue. Why? Because children and individuals do not react uniformly to these chemicals. There is a spectrum of symptoms and a varying degree to which people react from slight to severe. Studies do not take into account genetic, biochemical or nutritional individuality. Despite this, the studies are showing that there is a link between food chemicals and behaviour worthy of further research.
A 2012 review, Artificial Food Colors and Attention-Deficit/Hyperactivity Symptoms: Conclusions to Dye for, summarised the research on the topic. In the authors concluding remarks “While awaiting the results of such further research, the following conclusions seem reasonable”:
- “AFCs are not a main cause of ADHD, but they may contribute significantly to some cases, and in some cases may additively push a youngster over the diagnostic threshold”
- “By affecting nutrients and other metabolism in the periphery, AFCs could affect the brain without crossing the blood-brain barrier”
- “The deleterious effect does not appear to be confined to ADHD (a general effect has been replicated). Therefore AFCs may be more a general public health problem than an ADHD problem”
- “The magnitude of reported effect is reminiscent of subclinical lead poisoning (<10 mcg/dL) after correction for social factors, which led to the eventual removal of lead from gasoline”
- “There may conceivably be a possible deleterious effect on classroom climate from most children deteriorating slightly, thus additively or even synergistically impairing the learning atmosphere” (an interesting comment, and I would add to the family atmosphere as well)
- “The current status of evidence is inconclusive “but too substantial to dismiss.” Until safety can be better determined, we suggest minimizing children’s exposure to AFCs. With the current concerns about childhood obesity, there appears to be no need to make food look more attractive than its natural color”
The Southampton Studies
If that is not enough for you as a parent to take artificial food colours seriously, let’s take it to the next level. The above review paper referred to research from Southampton University, The Southamptom Studies, where children were challenged with a mix of artificial food colours. The colour additives included in the study, sometimes referred to as the “Southampton Six” were sunset yellow (E110), carmoisine (E122), tartrazine (E102), ponceau 4R (E124), quinoline yellow (E104) allura red AC (E129) and the preservative sodium benzoate (E211). It is interesting to note that the children were challenged with a total of 20mg of artificial food colours. Whereas in the table above it is estimated that the daily consumption in 2010 is over 60mg of artificial food colours!
The results “showed a small significant effect for all children, not just those meeting criterion A of DSM-IV ADHD. This suggests that food AFCs are more of a public health problem than an ADHD problem.” In other words the study showed that adverse effects from these food additives are not restricted to children with extreme hyperactivity associated with ADHD, but could also be seen in the general population. The significant adverse effects observed included inattention, impulsivity, tantrums and slow progress at school. Soon after the publication of the trial, Britain’s Food Standards Agency issued a warning urging parents of hyperactive children to avoid foods with multiple additives.
Parents should be aware that these studies are all short-term studies looking at the adverse effects of these chemicals. I am not aware of any long-term studies on what these chemicals may be doing, especially in young growing children. Critics of the Southampton study have said that it was a combination of food colours given so we do not know which individual component was causing the issue. However, testing combinations of food additives is logical, given this is how they are consumed by children in confectionary and other food items.
The negative effects of combinations of food additives are not well understood. In one 2006 study, compounds like MSG, aspartame, food dyes such as Quinoline yellow, and Brilliant blue were assessed and shown to exert significant synergistic neurotoxicity in the laboratory, and animal studies indicate that combinations of these additives are potentially more toxic than what might be predicted from individual compounds.
The Southampton studies prompted the UK and US governments to make changes to limit or remove these additives from children’s diets. However the evidence from the Southampton study wasn’t enough for food regulatory authorities, including those in Europe and Australia to make any changes.
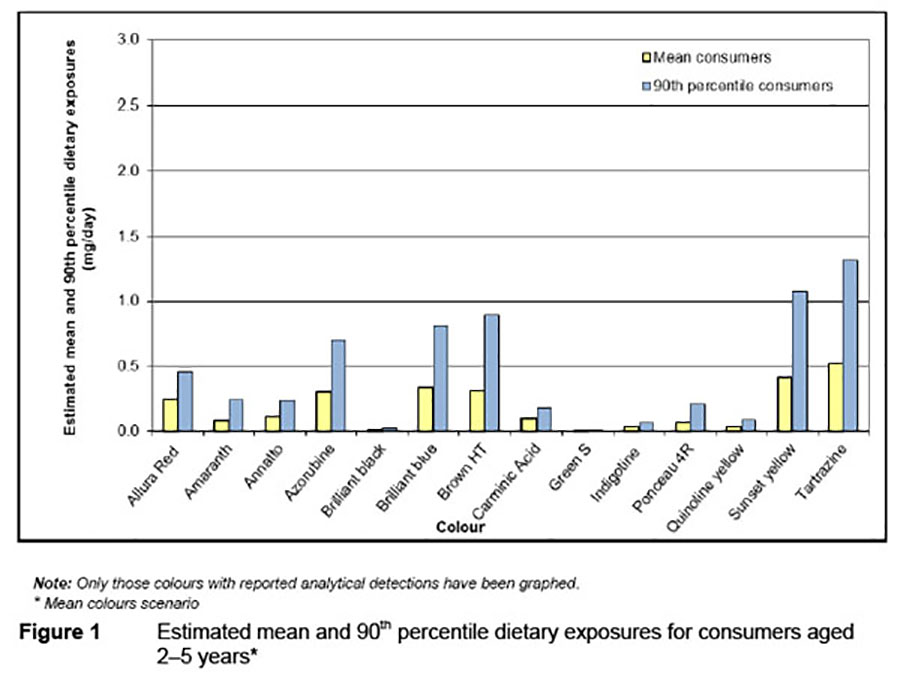
Source: Supplementary report to the 2008 survey of added colours in foods available in Australia.
The above graph is an estimated dietary intake of added colours in 2 – 5 year old children in Australia. The report is from 2008, so we can safely assume that children’s intake of dietary colours has increased since then. It is interesting that the estimated total intake reported is substantially less than from the 2012 study table at the beginning of this article. The graph below shows the items that were included in the Australian evaluation. I am surprised to not see processed meals included, unless it is included in “All other foods”. By processed meals I would include the frozen convenience foods reheated at home or purchased as takeaway meals. Items like crumbed foods (chicken nuggets, fish fingers), pizza, kids meals, etc. The graph below does show how widespread the use of food colours are in processed foods.
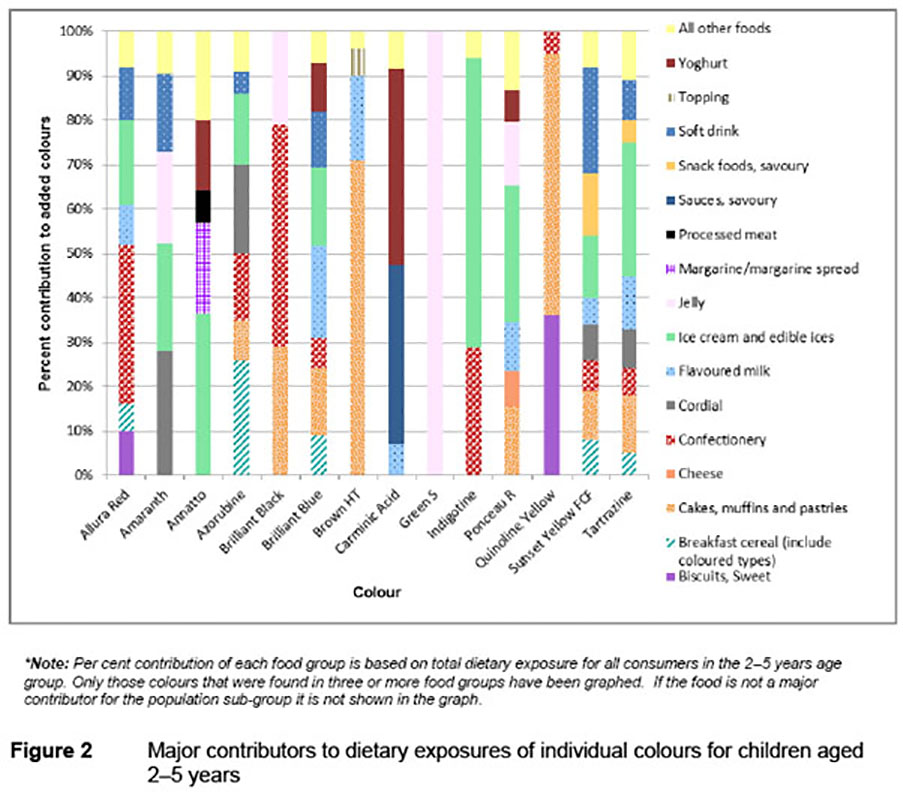
Source: Supplementary report to the 2008 survey of added colours in foods available in Australia.
Artificial Colours Banned Overseas But Allowed in Australia
From the Food Intolerance Website – Artificial colours around the the world, all the colours listed in the Southampton study banned in other countries, are allowed to be used in Australian food manufacturing.
- Sunset yellow [E110] – banned in UK, EU, previously banned in Norway
- Carmoisine [E122] – banned in UK, EU, USA, Canada, Japan, previously banned in Norway
- Tartrazine [E102] – banned in UK, EU, previously banned in Norway. This food colouring has well documented hazardous effects. Reactions can vary from mild to severe. Laboratory studies have shown that Tartrazine has clear immunosuppressive effects. Cases of skin eruptions in children have been reported. One published case report in a 5 year old girl showed that she suffered from recurrent reactions to this colorant, which included itchy skin rash, headaches, difficulty breathing, abdominal pain and loss of consciousness.
- Ponceau 4R [E124] – banned in UK, EU, USA, previously banned in Norway
- Quinoline yellow [E104] – UK, EU, USA, Japan, Canada, previously banned in Norway
- Allura red AC [E129] – banned in UK, EU, previously banned in Norway
- Sodium benzoate [E211] – a preservative used to inhibit the growth of yeasts, fungi and bacteria. This compound has been a subject of concern in the past. When mixed with vitamin C in soft drinks it forms benzene, a carcinogenic substance. There is evidence that sodium benzoate can damage and inactivate vital parts of DNA in a cell’s mitochondria. (Nutrition Care Bulletin. Vol 15, Issue 5, 2007)
In the EU, foods containing the Southampton Six colours have to carry the warning: “may have an adverse effect on activity and attention in children”.Health concerns about Brilliant Blue have also been raised by a laboratory study showing that Brilliant Blue may interact with other additives such as MSG to interfere with the development of the nervous system.
Individual Susceptibility
Not everyone is susceptible to the effects of food colourings and additives, and not everyone is affected in the same way. One person may display hyperactive behaviour while another may develop a migraine. However, young children are particularly vulnerable to the effects of food colours and additives. High exposure during the early developmental years can lead to behavioural and learning problems in later life. Exposure to toxic chemicals may directly or indirectly attack their undeveloped nervous, immune and endocrine systems (REF). Exposure during this vulnerable developmental period may be why we are seeing an increased incidence of allergy or hypersensitivity, and susceptibility to autoimmune and other conditions as the population ages.
We should never lose sight of the fact that exposure to food additives, as well as to toxic environmental chemicals is a concern not only for the very young, but for the majority of healthy individuals as well.
Concluding Remarks
Being in practice it is a real buzz to see parents after they have done a trial Failsafe or Royal Prince Alfred Hospital elimination diet and challenge, walk in and say “I have my child back again!” or “He is so much calmer and sleeping better. We can actually go out as family without the arguments.” Conversely, I also see parents that are not willing to consider or partially do a 2 to 3 week elimination diet and challenge and say there was no difference. If you are going to do this, you need to commit and do it strictly, or not at all. Some children do not show any change in behaviour or other symptoms. Yes, not all children will respond but it is a good starting point. Parents need to seriously weigh up the benefit versus inconvenience of doing an elimination diet, compared to the benefit versus risk of long-term medication and the possible future consequences.
All parents have the right to their own individual journey with their child/children. I am just showing you the door via my personal experience and the research studies that are being published.
Look and you will find it — what is unsought will go undetected” — Sophocles, Oedipus Rex, 429 BC.
Final thoughts to parents:
Don’t say in years to come that I didn’t know, the evidence is there, it has been for years AND is getting more convincing.
The sooner you do an elimination and challenge, the easier it is. Dealing with a young oppositional child is easier than dealing with an oppositional teenager. Modifying a diet is cheap, the benefits can be great.
The long-term effects of artificial food chemicals are still not known. Why would you want to knowingly give these chemicals to your child!
If you don’t try a strict elimination diet, don’t say it doesn’t work.
If an elimination diet doesn’t work (which may also include exclusion of gluten and or dairy), something else is a problem. You need to investigate further and consider lead, iron, yeast, Clostridia, neurotransmitter levels via an Organic Acid Test, behavioural therapy, screen time, etc. Most children’s issues are NOT due to a lack of Ritalin or other psychotrophic drugs!
No intervention is 100%, even medication!
Parents concern for their children’s wellbeing and future health should be 100%.

