
Articles appear regularly in print, media or the internet as to how parents are being taken advantage of by practitioners, that are peddling “quack therapies”, that are useless and even “dangerous”. It is scandalous that ASD children with underlying medical, nutritional and neurological issues that we are trying to help, are on the other hand being dismissed by mainstream medicine due to their autism diagnosis. Interestingly, even positive reports of ASD children who have improved significantly through diet, supplements or other therapies are not seen as offering much hope in the ASD community.
Unfortunately, positive research into non-pharmaceutical treatments for ASD does not make headline news as it does for other medical conditions. Headlines like Autism: Parents targeted by pseudo-medical charlatans with bogus treatments appear all too frequently. This is not intended to single out this one article as there are many that pop up on a regular basis. However, seeing yet another headline like this, and the perception that the autism research we are attempting to implement, are bogus treatments peddled by charlatans, it is time to make a statement. There is a reason why I have been following the latest developments in autism research for over 20 years. That is because I care, and I choose to be informed and NOT misinformed.
Firstly, let’s make it clear I do not treat autism. I do treat individuals with autism. There is a difference.
We do know that ASD individuals do have:
- Gastrointestinal issues
- Restricted diets and nutritional deficiencies
- Sleep disturbances
- Anxiety and mood disorder
- Obsessive compulsive issues
- Seizures
- Biochemical abnormalities
And the list continues.
A parent does not need to read research to know that if their child is constipated and not sleeping well, their child’s behaviour will be affected. The research does tell us that if a child develops aggression, self-injurious behaviour, then pain or discomfort is often the underlying cause. If you read the research and listen to parents with ASD children, over the years you realise that this is the only way these children can communicate to us that they are in discomfort. Unfortunately, mainstream medicine does not see it this way and still sees autism as primarily a neuropsychiatric issue rather than a medical disorder.
Any experienced biomedical practitioner should always look for signs and symptoms of underlying medical conditions and treat them accordingly. The article below is just one of many published research papers that is ignored by mainstream medicine. No interest in being picked up as newsworthy by the general media. Hence, it is easy to convince parents that anything other than behavioural therapy or pharmacological options are “bogus treatments”.
So what about these claims of bogus treatments? It’s like an urban myth, the majority believe it, but the reality is that it is not true but nobody bothers to check if it is true.
Dietary Modification in ASD
Let’s start with this ongoing controversy and headlines like the one below.
“Claims to minimise autistic traits”. Implication is that the diet should minimise autistic traits in all children. No, not all children’s autistic traits are improved on a gluten free, casein free (GFCF) diet, but a sub-group of children do improve significantly. Often there are improvements in bowel function, which in turn may have a beneficial effect on behaviour.
“No good scientific evidence.” There is good evidence that a sub-group of ASD children do well on a GFCF diet. Identify these individuals, redo the study, and you will come to a different conclusion. I have covered this in depth in a previous article which I encourage you to read research.
Supplements for ASD Individuals
How do we determine which supplement will best suit a child? There are indications from the medical history, like tiredness, poor muscle tone and anxiety that indicate which supplements would be most suitable. There are physical signs that also may indicate that there are deficiencies in iron, zinc or essential fatty acids. This can be confirmed by doing some testing like blood work (may be difficult, but some blood collection centres specialise in bleeding children), urine via an Organic Acid Test or a Hair Mineral Analysis test. It depends on each individual child, as to which test or tests would be appropriate. Twenty years ago, these tests were not readily available, therefore I was guided by the parent survey collated by the Autism Research Institute, as to what option may be useful for my child. The survey is as relevant today as it was 20 years ago.
Studies do show that ASD individuals have more nutritional deficiencies than the general population.
Dietary Patterns of Children with Autism Spectrum Disorder: A Study Based in Egypt.
Studies also show that nutritional supplements can generally manage autistic symptoms better than medication.
Micronutrients Versus Standard Medication Management in Autism: A Naturalistic Case–Control Study.
Conclusion from the study above:
“There were some advantages to treatment with micronutrients—lower activity level, less social withdrawal, less anger, better spontaneity with the examiner, less irritability, lower intensity SIB [self-injurious behaviour], markedly fewer adverse events, and less weight gain. Advantages of medication management were insurance coverage, fewer pills, and less frequent dosing.”
No media headlines here! So parents have no idea that this research exists.
Targeted Supplements for ASD Individuals
From the onset I would like to make it clear that we only consider supplements AFTER we deal with the major issues that may be causing an issue for a child. Constipation, loose stools, pain, discomfort, seizures, food intolerances, and so forth. You will never know if a supplement is useful if they are hyper and flying high as a kite on artificial colours and additives or are aggressive and can’t focus because they are in pain or discomfort. These issues need to be identified and dealt with FIRST. We don’t claim to “reverse autism”, we do supply nutrients, either through diet or supplements, for children to be able to grow and develop properly. In the process nature takes over and does the healing necessary for them to achieve their full potential in life.

“No double blind studies to prove worth.” Again, autism is a disorder with a wide spectrum of presentations. Just like individuals presenting with fatigue. There is mild fatigue due to late nights and eating crap, to low iron, thyroid issues, adrenal fatigue, insomnia, viral infections, pain causing more severe fatigue and chronic fatigue as we see in Chronic Fatigue Syndrome. Doing a study recruiting individuals with a broad range and severity of autistic traits (including intellectual disability), is different than doing a study on a specific well defined sub-group of ASD individuals (i.e. fatigue due to iron deficiency). Supplementing iron to all individuals with fatigue, compared to supplementing only those individuals that have been tested for low blood iron levels, would the study results be different in both groups? They obviously would be.
Despite the negative headlines for supplements, why are there reports that between 50 to 80% of children are on some sort of supplement?
“Approximately half of children and adolescents with autism spectrum disorder use complementary and alternative medicine. Doctors should be aware of this and should discuss complementary and alternative medicine use with patients and their carers, especially as the evidence is mixed and some complementary and alternative medicine treatments are potentially harmful.”
It is unfortunate that complimentary medicines that have been shown to be effective are reported as “potentially harmful”, yet pharmacological medications like atomexatine, as in this recent study are reported as appearing to be “safe and effective”. There is an obvious bias in the reporting of these studies.
On the issue of the quality of the studies using supplements in ASD, I have more faith in the quality of supplement studies than I do in the quality of pharmaceutical studies. Just read my recent article on the quality of the studies into antidepressants, which was the basis for antidepressants being accepted by the FDA for approval.
I do have a problem with the quality of supplements that are available on the market. Parents need to be aware that the majority of supplements on the market are of very poor quality. We are now even seeing “gummy bear” supplements for adults. Really? Read the sad state of the supplement market in the article Supplements – Buyer Beware, and only purchase supplements of the highest quality. Then you may see the results that you expect.
Let’s look at some of the studies into nutritional supplements and ASD that have been published.
Multivitamin – Mineral Supplement
In the following study two thirds of children showed improvements in many areas on a multivitamin-mineral supplement. This study is noteworthy as the supplement was formulated specifically for the study. Therefore, the quality of the ingredients used in the supplement were of the highest quality. Also the ingredients used in the supplement targeted many of the deficiencies that previous research has identified in ASD individuals.
Vitamin/Mineral Supplements for Children and Adults with Autism.
“about 1/3 of the group had no improvement, 1/3 had some improvement, and 1/3 had substantial improvement. The improvements were greatest in the group under age 18, but there were some reported benefits in the adult group as well.”
The graph below provides a summary of the results.
Looking at these results, if your child happens to be one of the two third of children that improved, would it be worth it? Could you justify the cost?
Omega-3
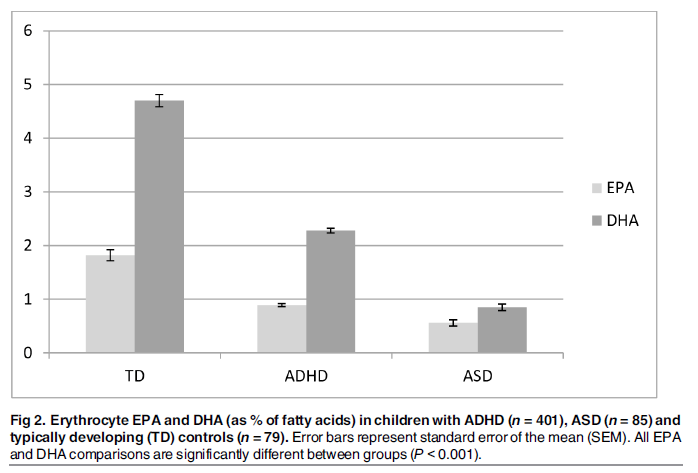
This study found lower levels of omega-3 (EPA and DHA) in children with ADHD and ASD compared with typically developing controls.
“As expected, lower levels of DHA, EPA and n-3/n-6 ratio and higher AA/EPA ratio were correlated with greater severity of symptoms.”
It is also noteworthy that: “Dietary supplementation with Bifidobacteria has been shown to increase tissue levels of EPA and DHA in mice, and dietary supplementation with parent n-3 PUFA alpha-linolenic acid (ALA) combined with Bifidobacterium breve resulted in higher liver EPA and brain DHA levels.”
There is a New Zealand trial currently in progress into vitamin D and omega-3 supplements, the results of which will be very interesting once they are published.
Folic Acid
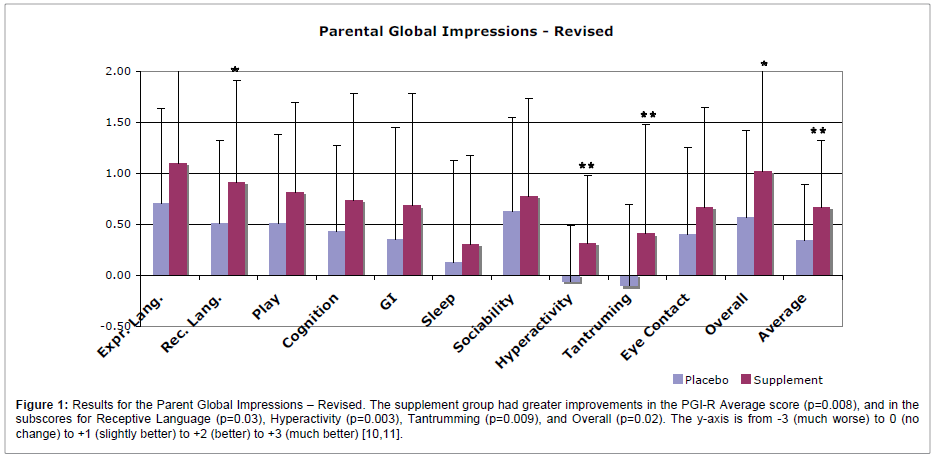
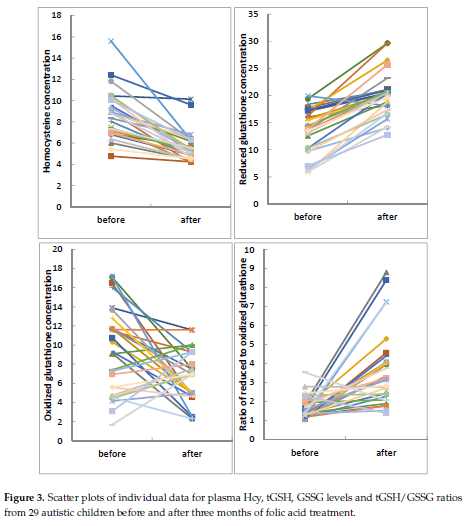
This study demonstrates that a three-month folic acid intervention in autistic children participating in structured teaching, significantly improved symptoms of autism in regards to sociability, cognitive verbal/ preverbal, receptive language, affective expression, and communication.
The study also showed altered the concentrations of folic acid, homocysteine (Hcy), and normalized glutathione redox metabolism. “These results unravel that children with ASD—or, at the very least, a subset of children with ASD—could benefit from this simple and safe nutritional supplementation.”
Although these results are useful, it would be even more useful to repeat the same study in ASD individuals in which their MTHFR gene mutation is known. Such a study may show significantly better results in the group with the MTHFR mutation.
Coenzyme Q10
Coenzyme Q10 is often used to help with mitochondrial dysfunction. Mitochondrial dysfunction has been shown to be an issue for a significant proportion of ASD individuals.
Ubiquinol Improves Symptoms in Children with Autism.
“Ubiquinol (CoQ10) supportive therapy improved symptoms in children with autism, as communication with parents (in 12%), verbal communication (in 21%), playing games of children (in 42%), sleeping (in 34%), and food rejection (in 17%).”
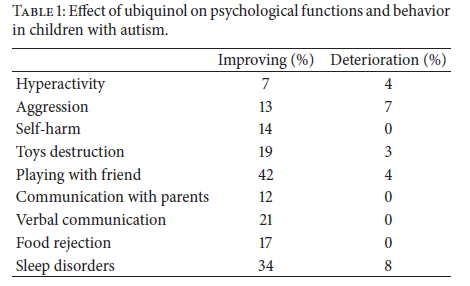
Yes, the percentage of children improving on coenzyme Q10 isn’t in the high percentages, but wouldn’t it be worth a 2-month trial and see if there is an improvement in your child? Would you be happy with any other treatment if you managed to get some of the improvements as seen above? For me as a parent I would be willing to give it a go for 2 months. Can we identify which sub-set of children may improve with coenzyme Q10? Yes we can, either through an Organic Acid Test or even genetic testing, as there are some gene defects that increases an individual’s requirement for coenzyme Q10.
N-Acetylcysteine
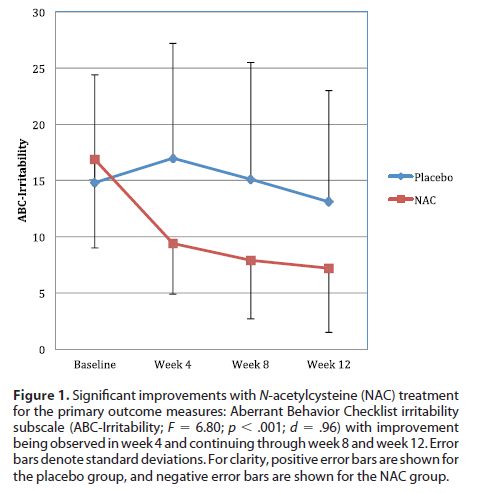
In ASD individuals that exhibit aggression, tantrums and self-injurious behaviour, this is certainly a supplement that I would consider. However, even before considering this supplement I would be asking the question, “What is driving the aggression and self-injurious behaviour?” Is there an underlying co-morbid medical issue that is causing them pain or discomfort? Again the graph below shows an improvement in symptoms within 4 weeks, and ongoing improvement at the 12-week mark. How many other therapies show such an improvement in 4 weeks?
A Randomized Controlled Pilot Trial of Oral N-Acetylcysteine in Children with Autism.
“NAC was overall well tolerated and might be helpful in targeting irritability in children with autism. This finding is important because the current Food and Drug Administration approved agents have a propensity to cause serious side effects (weight gain, metabolic abnormalities, and tardive dyskinesia), which have limited their use considerably. Managing irritability, which can be manifested by aggression, tantrums, self-injurious behaviours, and anger, with an effective and safer agent can improve overall functioning in individuals with autism and alleviate burdens on the individual and family.”
Sulforaphane
Sulforaphane is an extract from broccoli sprouts. Its therapeutic effect is based on its potent activity in up-regulating genes that control oxidative stress, inflammation, DNA-damage, and radiation.
Sulforaphane treatment of autism spectrum disorder (ASD).
“A significantly greater number of participants receiving sulforaphane had improvement in social interaction, abnormal behavior, and verbal communication. Upon discontinuation of sulforaphane, total scores on all scales rose toward pretreatment levels.”
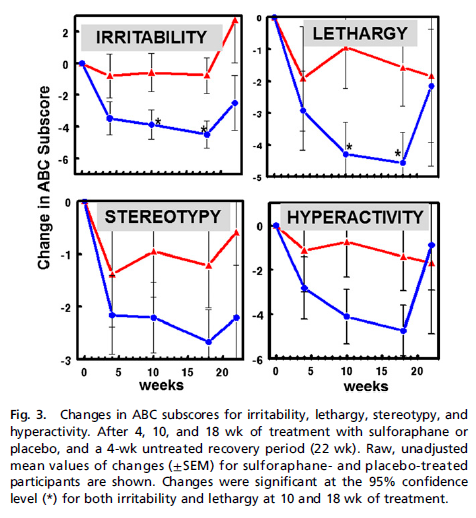
In a sub-group of ASD children, sulforaphane is showing benefit for irritability, stereotypy and hyperactivity. Worth a 4-month trial to see if it is effective for your child?
There are many other supplements and therapies that may be useful for a sub-groups of ASD children. It is the skill of the practitioner to know which ones may help your child or what tests to order that may indicate that there is an increased need for a particular supplement.
Before parents rush out and buy supplements to give to their children, here is a warning yet again. Supplements are big business and unfortunately there are many unscrupulous companies out there that do very little to ensure that they are supplying a quality product. As mentioned above I have written previously about the sad state of the supplement industry with poor or no testing of raw materials or the final product that is on retail shelves.
All supplements dispensed by my clinic are from companies that are proud to supply quality control data on every batch of supplements that they produce. For that reason, you can be assured that the supplements are of premium quality and you will get the results that you expect. Whenever research is published using a particular brand of supplement, if it is available in Australia, that is my first choice to use for your child.
Safety of Supplements
Supplements are continually touted as potentially “dangerous”. High quality supplements are safe.
Annual report reveals: No deaths from any nutritional supplements.
No Deaths from Vitamins, Minerals, Amino Acids or Herbs.
What is not safe is buying retail supplements of dubious quality or off the internet. Most adverse effects requiring transplantation are from weight loss, body building supplements or self-prescribed supplements bought off the internet.
Herbal supplements linked to at least six Australian organ transplants since 2011, data shows.
You can find more information on supplements here on my website.
Chelation
We continue to hear of reports of the dangers of chelation. Reports of deaths due to chelation. Yes, I have heard of these deaths and must admit never looked into the details of these deaths. Until now.
Firstly, intravenous chelation for children is not done here in Australia. So forget the $100/ treatment headline.
Next the two case studies in which children died as a result of chelation:
Deaths Resulting From Hypocalcemia After Administration of Edetate Disodium: 2003-2005.
Case 1: A 5-yo ASD boy
“In August 2005, a boy aged 5 years died while receiving 990 mg of Na2EDTA IV pushed over 5 to 10 minutes in a physician’s office. The child was receiving chelation as treatment for autism. The myocardial necrosis resulted from hypocalcemia associated with administration of Na2EDTA.”
In other words, this doctor used Sodium-EDTA instead of Calcium-EDTA as a very fast IV infusion. This resulted in rapid depletion of calcium and cardiac death. The WRONG form of EDTA was used together with a rapid infusion, which is NOT the recommended protocol.
Case 2: A 2-yo girl with lead poisoning
“In February 2005, a 2-year-old girl tested for blood lead during routine health surveillance had a capillary BLL [blood lead level] of 47 µg/dL. A complete blood count and iron study conducted concurrently revealed low serum iron levels and borderline anemia. On February 28, 2005, she was admitted to a local medical center for chelation therapy to reduce her BLL.”
“Initial medication orders included IV Na2EDTA and oral succimer. The medication order subsequently was corrected by the pediatric resident to IV CaNa2EDTA. At 4:00 PM on the day of admission, the patient received 300 mg of CaNa2EDTA in 100 mL of normal saline at 25 mL/hour IV. At 4:35 PM, she was administered 200 mg of oral succimer. Her vital signs remained normal throughout the night. At 4:00 AM the following morning, 300 mg of Na2EDTA instead of IV CaNa2EDTA was administered IV. At 7:05 AM, the child’s mother noticed that she was limp and not breathing. Cardiac compression and O2 via ambu bag did not restore a normal cardiac rhythm, and a cardiac resuscitation code was initiated at 7:25 AM. All attempts at resuscitation failed, and the girl was pronounced dead at 8:12 AM. The cause of death was recorded as sudden cardiac arrest resulting from hypocalcemia associated with chelation therapy. The hospital’s child mortality review board findings indicate that a dose of IV Na2EDTA was unintentionally administered to the child.”
Both deaths were due to IV Endrate (sodium-EDTA) infusion which was inappropriate and due to PHYSICIAN and HOSPITAL ERROR!!
Chelation is not dangerous. Except if the wrong chelating agent or chelation protocol is used.
Period!
Now to address the statement “A large study in 2008 was stopped by the regulating authority in the US because of the dangers associated with it.” An explanation in the following article explains the basis on which the chelation trial was stopped.
Chelation: Harnessing and Enhancing Heavy Metal Detoxification—A Review.
“A trial of chelation therapy to treat autism registered on the US National Institutes of Health (NIH) http://www.clinicaltrials.gov website is indicated as “completed,” with the last update October 13, 2009 [91]. When contacted for an update, the NIH representative replied that the trial had been cancelled before recruitment, because some adverse effects were observed in a study of 120 rats [92]. This study by Stangle et al. clearly demonstrated that a single three-week course of high dose DMSA treatment ameliorated learning, attention, and arousal regulation in rats exposed to lead during a period from early postpartum to late adolescence. The treatment also reduced lead levels in both the blood and brain. What prompted cancellation of the autism trial was detection of a potential adverse drug effect in the form of adverse cognitive effects among unexposed rats [to lead] that were treated with DMSA, compared with unexposed, untreated rats.”
“This pivotal animal study led to cancellation of a large, much-publicized trial in children.”
“In the Stangle et al. study no mineral supplementation was provided, and no minerals other than lead were analysed. DMSA is well known to enhance excretion of many elements, notably zinc [93]. Zinc deficiency impairs neurocognitive development in the young [94, 95]. In addition, Stangle et al.’s rats were treated using an “aggressive” protocol, with 50mg/kg/day DMSA for 21 days; a dose that is much higher than the US Food and Drug approved maximum label dose of 30mg/kg/day [93], that is typically used for less than a week at a time in children [96]. It is probable that detrimental effects attributed to DMSA resulted from deficiency of essential elements, an effect that is eminently avoidable.
In summary, the Stangle et al. study violated important current clinical practices by administering the drug at a high dose, over an extended period of time, when there was no indication of need; and failing to assess essential minerals loss and ensuring that minerals were appropriately supplemented to avoid health consequences.”
Reading the above review, sheds a completely different light on the danger of chelation in children! This is what happens when an urban myth is circulated and nobody bothers to check the credibility of the statements. Lazy journalism!
Applied Behavioural Therapy (ABA)
Applied Behavioural Therapy is widely used and endorsed as a scientifically proven and effective treatment. However, the reason why I have mentioned it here is that there was a study that was published recently Perceptual learning in autism: over-specificity and possible remedies, which parents should take note of. This study published in Nature Neuroscience shows that training individuals with ASD to acquire new information by repeating the information actually harms their ability to apply that learned knowledge to other situations. This finding, by an international research team, challenges the popular educational approaches designed for ASD individuals that focus on repetition and drills. The individuals with autism performed poorly when the target location was changed and they were not able to improve their performance, indicating that they received no benefit from initially learning in the first location. Even more interesting, they were never able to learn in the second location as well as the first, demonstrating an interference in learning that may reflect the consequences of extensive repetition.
In other words, teaching ABA only in one setting is detrimental to transferring what they have leant to situations outside the ABA setting. Parents I have spoken to have noted the same thing. Their children do well in the ABA setting, but are unable to transfer these skills outside the ABA setting. The implication is to do ABA in a variety of settings, so that the child is able to transfer learnt skills outside of the ABA setting. There was some criticism from ABA practitioners about the study. However, as a parent I would be taking note of the findings.
I “Cured” My Child of Autism!
Finally let me say something of the headlines like “I cured my child of autism with (insert here the plethora of different diets, supplements and other interventions)”. They should be an inspiration to other parents. However, there is a part of the autism community that does not react positively to such reports. Parents should be aware that there is a proportion of parents that have done what they can, but despite their best efforts, their child has not progressed significantly. For the sake of balance, I also include the following article:
Why Autism SuperMoms Make Me Feel SuperBad
“So, I guess maybe I’d be totally ok with all these autism super moms and all these autism miracle stories if they all came with a disclaimer. The same disclaimer they put in tiny print on late night infomercial diet and acne medicine commercials.”
“It drives me crazy, but parents need to be told what is evidence-based. We pay a lot of money to people who don’t produce results.”
In reply to statements like the one above, parents often listen to (and do not question) mainstream doctors who are not interested in, nor follow evolving ASD research. If you want to be informed, you need to look for the research yourself. It’s not hard, I have a monthly summary of ASD research on my Autism page on my website. Mainstream medicine will tell you what they want you to hear, not what you need to hear. Evidence based medicine is there on the internet for everyone to see. You just need to know where to look. Gone are the days where the research was only in printed journals, and only available to doctors on subscription. Now the information is out there and can’t be “hidden” on doctor’s shelves as it has been in the past.
“We pay a lot of money to people who don’t produce results.” – I totally agree! How much money do parents spend on paediatricians, behavioural paediatricians and psychologists per consultation? How happy are parents with the advice that they have received from their paediatrician or psychologist? Probably the biggest complaint from parents is that their concerns about their child are not listened to. “Why do I spend so much money per consultation and get noting out of it for my child?”
Maybe the final word about the cost of biomedical treatment is best put into perspective by a mother with children on the spectrum.
“Don’t for a minute think that all integrative doctors and complementary therapists are more expensive than mainstream treatments. The difference is that they are not being propped up by the government. Your local gp rates are in order of $60.00 for 10 minutes-that’s $360.00 an hour! Of course you never know that because its paid through the back door by taxes that I contribute to…and 10 minutes is nowhere near enough for comprehensive health care so back you go tomorrow and the next day and the day after that and so on -ultimately spending many taxpayer dollars.”
“Not all therapies have worked for us but I can tell you this-NONE have harmed him. People die or are harmed or at the very least are not helped by mainstream medicine all the time, but this is constantly overlooked-again.”
Concluding Comment
Yes, not all children respond as quickly as we would like. Occasionally I will have parents come back after one or two visits and say, “No I don’t see any difference in my child with what you have recommended”. I make a point of taking an extensive medical and symptom summary for each child. In these cases, where parents do not see a difference in their child, I ALWAYS review the list of symptoms and medical issues that the child first presented with. Invariably as we review the list the parent will say that, yes there are actually improvements in their bowel habits, sleep, concentration, anxiety, or some other behaviour. Parents are with their child 24/7 so don’t always see the small changes that healing is about. Those that don’t see the children as often are more likely to pick up these differences. Sometimes when we address the biggest issue facing the child we get the “wow” moments. More often than not it is a more subtle process, as each child is individual and time is needed as we heal the gut, inflammation, cell membranes, replace depleted nutrients, correct biochemistry, support detoxification and optimise nutrition. As one parent once said, healing an ASD child is a “marathon, not a sprint”. It is a long process and involves many different therapies, nutritional intervention is only just one. Yes, they still have their autistic traits, BUT you may be able to take them out without them having a meltdown, they are able to concentrate during therapy, they can sleep through the night, and so forth. At least you are seeing some positive progress. For those parents that have tried these interventions and they did not work, or they did not get the results that they expected, then unfortunately their child is in the sub-group for which these did not work. However, there are many ASD children for which they have worked and they have improved considerably. As a result it has also made a huge difference to their families quality of life.
There is NO intervention, diet or supplement that works for ALL ASD children. But ALL children should be comprehensively investigated for underlying co-morbid medical issues that are treatable.
